Koren Rumelia1, Bumbuluţ Călin2, Rath-Wolfson Lea1
1Department of Pathology Hasharon Hospital, Rabin Medical Center, Petach Tikva and Sackler Faculty of Medicine, Tel-Aviv University, Israel and 2SCM Satu Mare, România
This paper was presented at the “Medical Days of Satu Mare” ,VI-th Edition, October 1-3, 2009, Satu Mare, Romania
Abstract
Background: Detection of metastatic lymph nodes (LN) in cancer disease is essential for determining stage and, thus, therapeutic modalities. However, very small LN can easily be missed during routine examination.
Objective: The aim of this study was to describe a new and easy technique for detecting tiny LN in colonic, breast, stomach and urinary bladder specimens. All patients were clinically free of distant metastasis (M0).
Methods: Fatty tissue from 30 surgical specimens of colorectal cancer, 13 axillary dissections, 10 from of gastrectomies and 12 cystectomies in which number of LN was unsatisfactory by traditional method, were investigated by Lymph Node Revealing Solution (LNRS) method. The entire fatty tissue was immersed for 6-12 hours in 3 times its volume of LNRS. The fatty tissue was washed thoroughly under running tap water and sectioned again at intervals of 2-3 mm. The LN stands out as white chalky structures on the background of the semitransparent fatty tissue. LN were excised, embedded in paraffin and stained with hematoxylin & eosin.
Results: LNRS helps to visualize even the smallest LN measuring 0.2 mm. These stand out as white chalky structures on the background of the semitransparent fatty tissue. In colorectal cancer specimens the mean number of L N increased from 10/88 to 37/346 and changed the N-stage in 18 of the 30 studied cases. In the axillary dissection cases the mean number of LN increased from 6/79 to 20/163 and changed the N-stage in 4 of the 13 studied cases. In the stomach cancer cases, there was an increase in mean of LN number, from 4/30 to 23/119 and changed the N-stage in 6 of the 10 studied cases. In the cystectomy cases the mean number of LN increased from 4/22 to 16/43 and changed the N-stage in 3 of the 6 cases.
Conclusion: LNRS is an easy, rapid and inexpensive technique for detecting very small LN. These may contain metastases, a fact which changes the stage of the disease and influences the therapy mode.
Key words: LNRS, cancer, colon, breast, stomach, urinary bladder
Detection of metastatic LN in pieces of cancer is essential for determining stage and thus, therapeutic modalities. However, very small LN can easily be missed during routine examination.
LNRS can be used after fixation in formalin whenever an unsatisfactory number of nodes has been sectioned. The smallest ones, of only a few millimeters, are evident even to the inexperienced residents coping with routine surgical specimens. Nodes are easily recognized as white nodules standing out clearly on the background of semitransparent fat (Fig. 1).
LNRS is a mixture of 65% of 95% ethanol, 20% diethyl ether, 5% glacial acetic acid, and 10% buffered formalin prepared under hood. It can be prepared extemporaneously in a hood, but it can be can stored in closed containers at laboratory temperature. It can be even reuse, but the efficiency decreases.
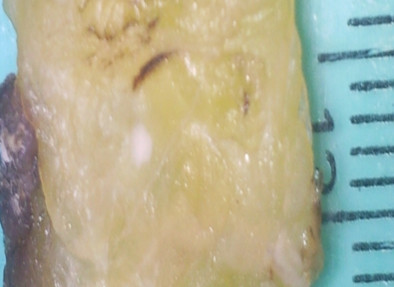
Fig. 1. LNRS treated fat, the lymph nodes appear as small white structures
In medical literature was described the LNRS method for lymph node detection, in colorectal specimens [1], also for mastectomy [2], gastrectomy [3] and total cystectomy [4], finding it very useful in improvement of N stady from TNM classification.
All patients were clinically free of distant metastasis (M0).
LNRS in colorectal cancer
All specimens showed mezocolon and perirectal fat depending upon the size of preparation and ability of the surgeon. One hundred cases of colorectal cancer were investigated prospectively. Specimens were fixed in formalin, after which fragments were taken for routine microscopic examination. LN of the mesocolic and\or rectal fat were searched for by the traditional technique i.e. serial sectioning, examining and palpating the adipose tissue. All lumps suspected of being LN were completely excised and processed routinely. From the 100 cases of colon cancer, 30 problematic cases in which the number of LN was considered unsatistactory: these included specimens with less than 10 LN and those with less than three metastatic nodes. Our criteria for assessing the unsatisfactory cases were in accord with the recommendations of „The American Joint Committee on Cancer (AJCC) staging system” which provides:
Nx – regional lymphnodes not assessed
N0- No metastatic lymph nodes
N1-1-3 positive nodes
N2- 4 ore more positive nodes.
So smaller difference between N1 and N2 entitles the method. In unsatisfactory cases, the entire mesocolonic fat was immersed for six to twelve hours in LNRS in approximately three times its volume of LNRS. Subsequently, the fat was washed thoroughly under running tap water and sectioned again at intervals of 1-2 mm.
After LNRS, the LN stood out as white, chalky nodules on the background of the yellow fat. (Fig. 1). They were then excised, processed and stained with hematoxyline and eosine (H&E). Their histological image can take a microscopic field at the examination with the 10 objective and eyepiece 10 of the microscope (Fig. 2).
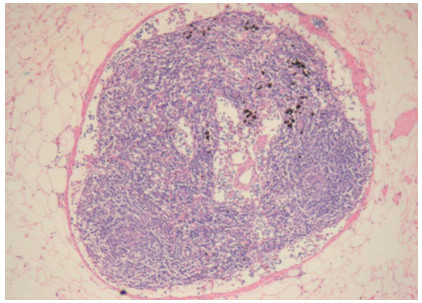
Fig. 2. Lymph node after treatment with LNRS, Haematoxylin & Eosin X100
Microscopic examination of the H&E stained slides after LNRS revealed normal architecture without distortion of the lymphoid tissue nor the metastases. After remounting in LNRS the histological sections of metastatic lymph, stained H&E presents the architecture of normal LN (Fig. 3) and of the metastasis, whitout artifacts. We distinguish the groups of epithelial cells of metastasis that replace the lymphatic tissue (Fig. 4).
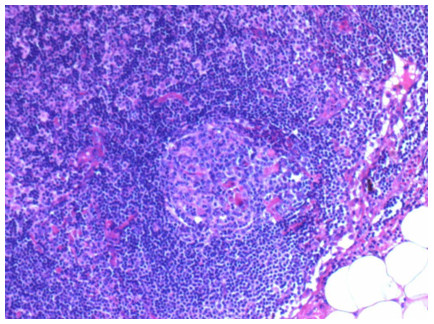
Fig. 3. Normal histological appearance of a lymph node after treatment with LNRS (H&E X200)
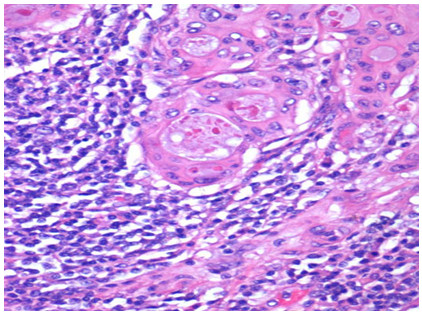
Fig. 4. Histological appearance of the metastasis of colon adenocarcinoma in a lymph node After treatment with LNRS (H&E X400)
The quality of immunohistochemical staining after treatment with LNRS is similar with those after formalin fixation (Fig. 5).
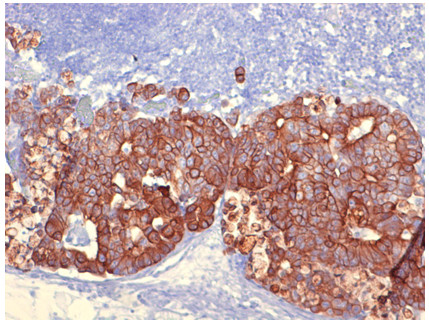
Fig. 5. Immunohystochemical staining psitive for cytokeratin in a case of metastasis of colon adenocarcinoma in a lymph node after treatment with LNRS (x200)
The number of LN found by the traditional method and with the LNRS was recorded, noting their size and the number with metastasis. Using the traditional method a total number of 88 LN was detected in all the 30 cases. After LNRS 258 additional LN varying in size from 0.5 mm to 7 mm, were found. The LN metastases increased from 10 with more 27 (Fig. 6).
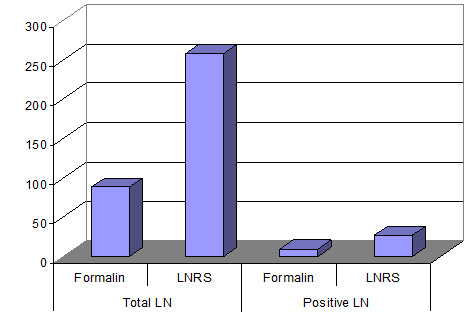
Fig. 6. Lymph nodes detected through the traditional method and LNRS in 30 difficult cases of colon and rectum cancer
The N stage was modiffied in 18 cases from 30; 8 Nx cases became N0, 4 cases considered previously to be N0 became positive (N1), and two cases previously graded as N1 became N2 after LNRS. We were able to upstage 8 cases from Dukes B to C (Fig. 7).
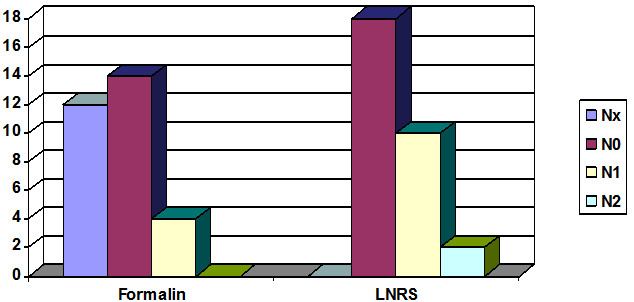
Fig. 7. Changing of N stage (TNM) in 30 difficult cases of colon and rectum cancer
The application of LNRS method in breast cancer
Were investigated prospectively 305 cases axillary dissection performed for breast cancer. In 13 of these were highlighted by the traditional method less than 10 LN, we have found difficult and we have included in our study. The adipose axillary tissue of these cases, after the excision of nodules by rutine method, were treated with LNRS for 6-12 hours.
From histological point of view there are two distinct histological types of breast carcinoma after ductal or lobular origin. The ductal origin carcinomas are: infiltrative ductal carcinoma and ductal carcinoma in situ. The latest presents small cells, often arranged in rows. Their detection in LN is difficult due to small size of epithelial cells, sometimes approaching to the size of a large lymphocytes. In common practice is required immunohistochemical staining for the safety diagnosis.
Macroscopically, the LN after remounting in LNRS were white, well defined against the background of yellow fat. Microscopically, the immunohistochemical staining for Citokeratin points the metastatic cells, colored in red on the background of lymphoid cells, stained only with hematoxylin. The staining with Leukocyte common antigen highlights in red the lymphocytes, while the remaining of metastatic epithelial cells remains unstained by the chromogen.
The number of LN examined were evaluated through each method.
The number of LN examined were evaluated through each method in the 13 axillary dissection for breast cancer. Through the traditional method of formalin fixation were detected 79 LN. Using LNRS after fixation in formalin were also detected 84 lymph more. The LN metastases increased from 6 with 14 more (Fig. 8).
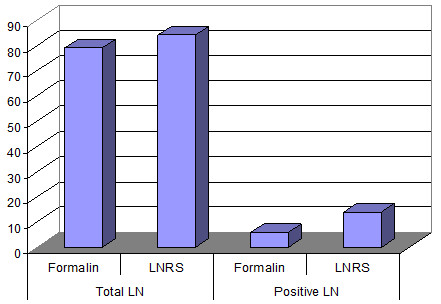
Fig. 8. The number of lymph nodes detected by the traditional method and LNRS in 13 difficult cases of breast cancer
LNRS has changed the N stage of disease in four of the 13 axillary dissection for breast cancer: in two cases from N0 to N1bi, in a case of Nx to N1bi, and last from N1bi in N1bii (Fig . 9).
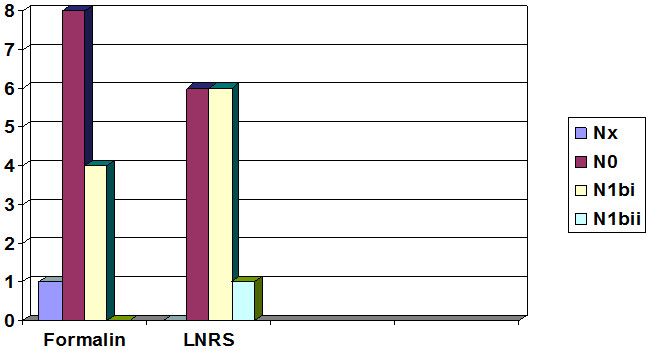
Fig. 9. Changing of N stage (TNM) in 13 difficult cases of breast cancer
LNRS method in gastric cancer
We considered unsatisfactory those gastrectomy in that were taken from the perigastric fat of each case less than 10 LN by the traditional method. Subsequently, the perigastric fat was treated with LNRS for 6-12 hours. Macroscopically it is striking the white aspect of LN. Microscopically, the PAS staining (Periodic Acid Shiff), which stains the mucopolyzaharides, is positive in a metastasis of undifferentiated adenocarcinoma and negative in adjacent lymph tissue. The number of LN examined were evaluated through each method. Through the traditional method of formalin fixation were detected 30 LN. Using LNRS after formalin fixation, were also detected 89 LN more and the number of LN metastases increased from 14 with 19 more (Fig. 10).
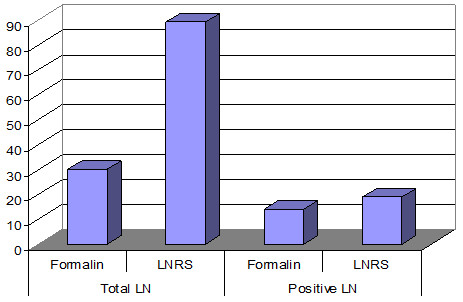
Fig. 10. The number of lymph nodes detected by the traditional method and LNRS in 10 difficult cases of stomach cancer
The N stage was changed in five of 10 cases: four cases classified by the traditional method Nx became N0 and in a case N1 became N2, after using LNRS method (Fig. 11).
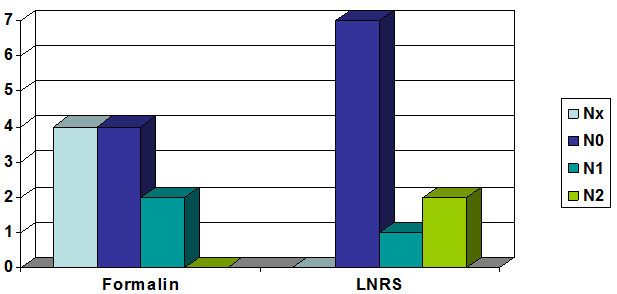
Fig. 11. Changing of N stage (TNM) in 10 difficult cases of stomach cancer
LNRS method in bladder cancer
Total cystectomies are relatively rare. Were prospectively investigated 12 cystectomies for transitional cell carcinoma (TCC). The specimens were fixed in formalin and LN in adipose tissue were harvested by traditional methods. Of these, six specimens in that were highlighted three or less than three LN were subsequently refixated with LNRS. The specimens from total cystectomies are pathological examinated immediately after removal, before the end of the operation. Probes are inserted through the ureteral orifices for directing the specimen, after which are open in the Y shape.
The number of LN examined were evaluated through each method.
Through the traditional method of formalin fixation were detected 22 LN. Using LNRS after formalin fixation were also detected 21 nodules more, and the number of LN metastases increased from 4 to 12 more (Fig. 12).
The N stage was changed in three of six cases: one case classified by the traditional method Nx became N2, one N0 N2, and another N1 case became N2 after the use of LNRS method. Graphical representation of the N stage in the six difficult cases of bladder cancer (TCC) shows the changed situation in the four N stages (Fig. 13).
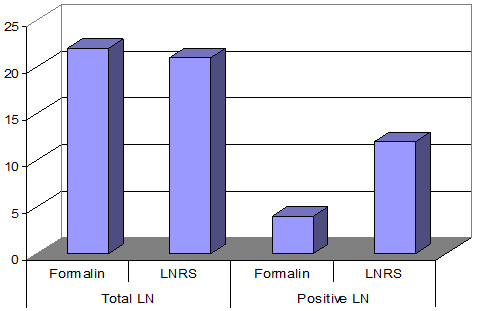
Fig. 12. The number of lymph nodes detected by the traditional method and LNRS in 6 difficult cases of bladder cancer

Fig. 13. Changing of N stage (TNM) in six difficult cases of bladder cancer
The data from literature confirm the fact that LNRS increases the total number of LN and the metastatic ones, also is effective in detecting the small LN. In general, the LNRS method is useful in the cases which presents an insufficient number of LN detected by classical method [5]. Salek and Haeri [6] found that in all cases classified as Nx (unidentified regional LN) through traditional method, were detected LN after LNRS method. The average diameter of thus dissected LN was significantly lower than the traditional method (0.268 vs. 0.429, p <0.000001). LNRS in comparation with other solutions is cheap, fast and easy to use. The authors of this study [6] propose the using of this solution in all cases Dukes B and in cases of patients which were not detected LN by the traditional method. Using LNRS [7] they also found an significant increase of number of LN detected, this can allow the examination of more than 12 in most cases in stage pT2, and pT3 in adenocarcinomas of the colon and rectum.
Conclusions: LNRS is an easy, rapid and inexpensive technique for detecting very small LN. These may contain metastases, a fact which changes the stage of disease and influences the mode of therapy.
Referrences
1. Koren, R, Siegal A, Klein, B, Halpern, M, Kyzer, S, Veltman, V, Gal, R. Lymph node-revealing solution: simple new method for detecting minute lymph nodes in colon carcinoma. Dis Colon Rectum. 1997;40(4):407-10.
2. Koren, R, Kyzer, S, Paz, A, Veltman, V, Klein, B, Gal, R. Lymph node revealing solution: a new method for detection of minute axillary lymph nodes in breast cancer specimens. Am J Surg Pathol. 1997;21(11):1387-90.
3. Koren, R, Kyzer, S, Levin, I, Klein, B, Halpern, M, Rath-Wolfson, L, Paz, A, Melloul, MM, Mishali, M, Gal, R. Lymph node revealing solution: a new method for lymph node sampling: results in gastric adenocarcinoma. Oncol Rep. 1998;5(2):341-4.
4. Koren, R, Paz, A, Lask, D, Kyzer, S, Klein, B, Schwartz, A, Gal, R. Lymph-node revealing solution: a new method for detecting minute lymph nodes in cystectomy specimens. Br J Urol. 1997;80(1):40-3.
5. Ustün, MO, Onal, B, Tuğyan, N, Rezanko, T. Lymph node revealing solution: is it effective on detecting minute lymph nodes? Adv Clin Path. 1999;3(4):135-8.
6. Saleki, S, Haeri, H. Lymph node revealing solution: A prospective study on 35 patients with colorectal carcinomas Acta Medica Iranica 2002;40(4):223-225).
7. Svec, A, Horák, L, Novotný, J, Lysy, P. Re-fixation in a lymph node revealing solution is a powerful method for identifying lymph nodes in colorectal resection specimens. Eur J Surg Oncol. 2006;32(4):426-9.

